Permanent pacemakers are the only long-term treatment for abnormally slow heart rhythms.
The very first permanent pacemakers used electrodes which were placed on the outside (Epicardial) surface of the heart’s chambers. Placing these electrodes was relatively invasive, as the rib-cage had to be opened to insert them.
Transvenous pacemakers solved this problem by using the body’s own veins (from the upper chest/shoulder) as conduits to place the leads onto the inner (endocardial) surface of the heart’s chambers. In widespread use for decades by now, these systems have been continuously refined to provide the highest levels of efficiency and durability.

This is a typical Pulse Generator (“Battery”) for a transvenous pacemaking system.
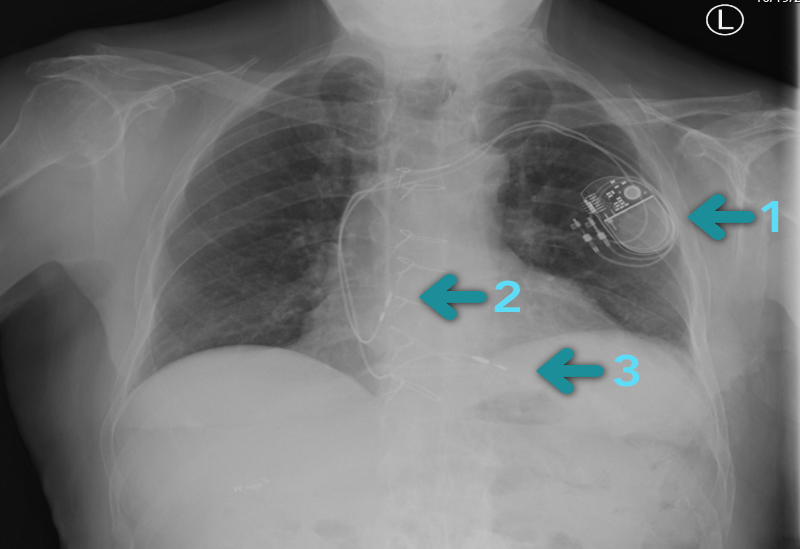
This chest X-ray demonstrates a dual-chamber transvenous pacemaker. Arrows indicate the Pulse Generator (1), plus electrodes in the Right Atrium (2) and Right Ventricle (3).
Certain medical conditions, (such as blocked veins in the chest or a recent serious infection) preclude the use of transvenous systems. Similarly, certain social circumstances (significant memory loss, behaviour issues) predict that a patient will endanger a transvenous system: incisional infection from poor wound care, lead dislodgement from inattention to arm restrictions for example. Rarely, a very young patient may have cosmetic concerns about the incision or pulse generator prominence. Leadless pacemakers are available for these special circumstances. Leadless pacemakers can be placed in either the atrium, the ventricle, or in both chambers for those would benefit from signal co-ordination.

Atrial and ventricular leadless pacemakers. Note the smaller size of the atrial unit, given that it resides in a smaller chamber.
Placed percutaneously using a multi-component catheter inserted through the femoral vein in the crease of the groin, these systems are entirely self-contained: the battery, circuitry and output channel are all in 1 small unit which is placed inside the heart chamber. 1 or 2 units may be used (one in each chamber) depending on the patient’s needs.
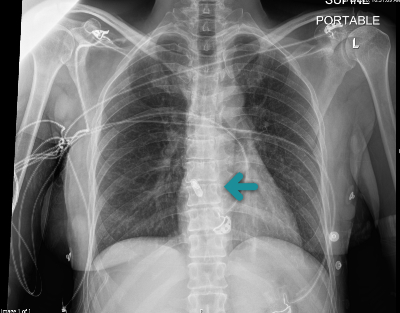
This chest X-ray demonstrates a leadless pacemaker in the atrial position. Note the size relative to the transvenous pulse generator in the earlier chest X-ray.
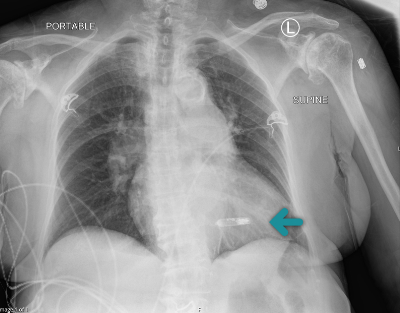
This chest X-ray demonstrates a leadless pacemaker in the ventricular position.
Despite the novelty and promise of Leadless systems, it must be remembered that they are a relatively new technology: expensive and without long-term data about their performance and battery longevity. Transvenous pacemakers are, in contrast, so well-refined over decades of development that they should be considered an apex technology: inexpensive, predictable in function, supremely reliable, with typical battery longevity of ten or more years. They continue to be the most appropriate system for the majority of patients.
