
Pulsed-Field Ablation
Catheter ablation is often the therapy of choice to permanently cure abnormally fast or irregular heart rhythms. The goal is the removal of abnormal electrical signals or electrical circuits within the heart. How this is done has evolved over the years.
Radiofrequency (RF) was the first catheter-based ablation and remains in widespread use today. This modality uses an electrical current to produce a local tissue temperature rise, effectively acting like micro-cautery. In this fashion, malfunctioning tissue is destroyed. For focal ablation, RF remains the standard of care.
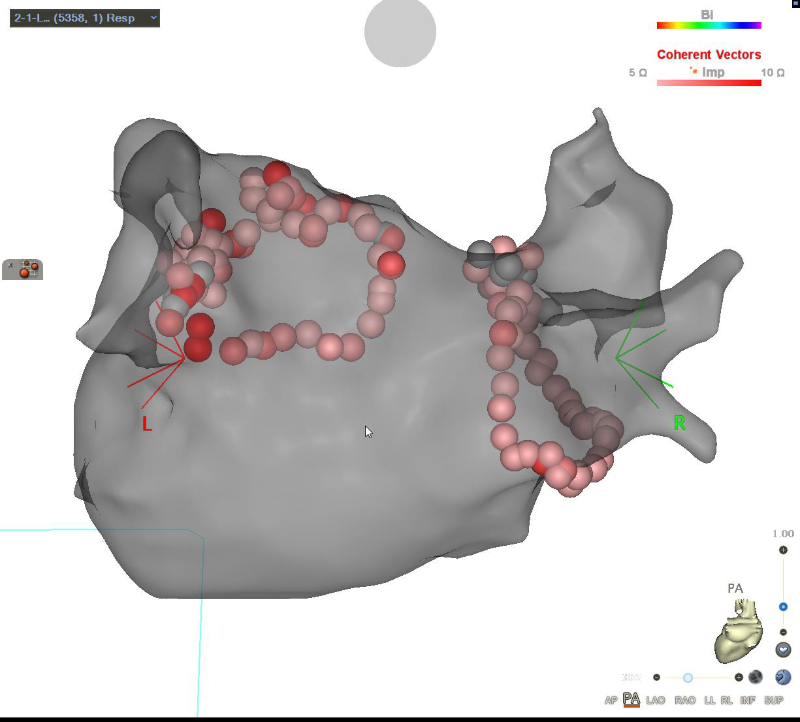
Here is a 3D electroanatomic map of the left atrium and its 4 pulmonary veins showing each of the RF lesions, represented as a red sphere. One can only imagine how time-consuming and arduous it is to place each of these ablation points, one by one, around the veins to completely encirclement. RF-based AF ablation has rightly begun to fade into history.
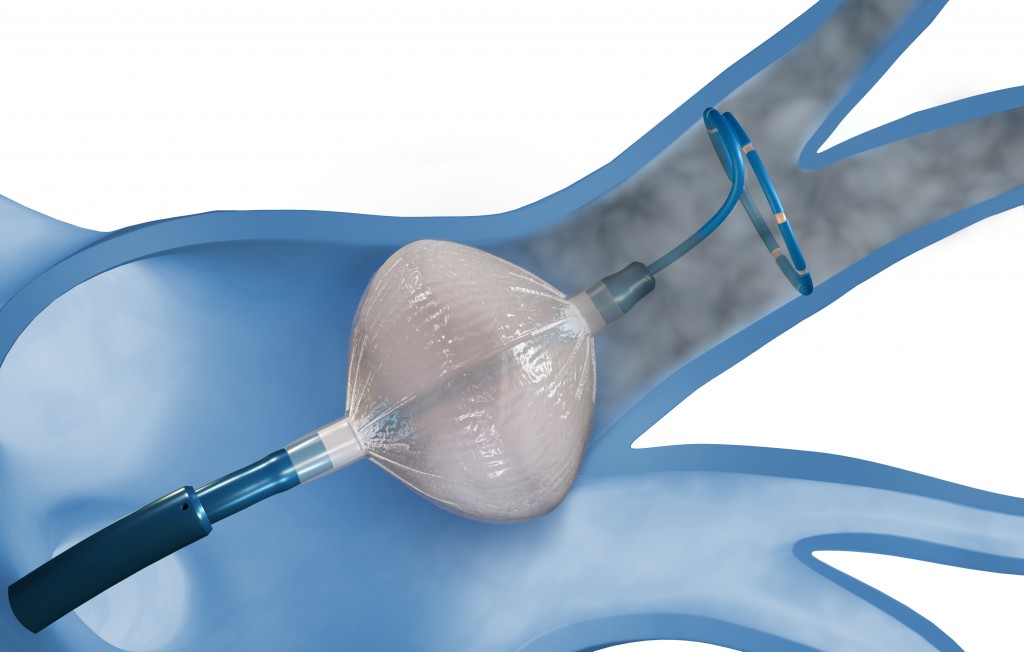
Cryoablation (Cryo) is a slightly more recent development, using very cold temperatures to “flash-freeze” tissue so that it loses its conductive capacity. Although cryoablation can be applied in point-fashion, it is most widely used in balloon-tipped catheters to treat the pulmonary veins in Atrial Fibrillation ablations.
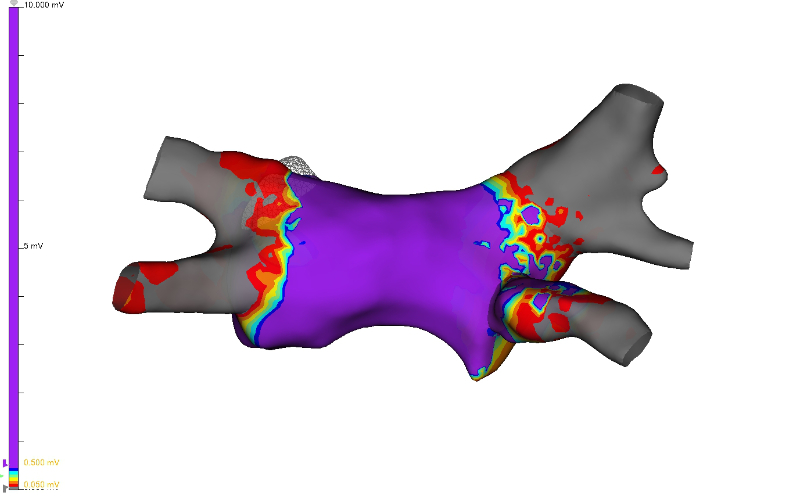
Here is a 3D electroanatomic map of the left atrium and the pulmonary veins after therapy with the cryoballoon. Note how each vein is readily encompassed by just 1 cryotherapy application, however, each vein is very narrowly ablated leaving much of the left atrial posterior wall electrically intact.
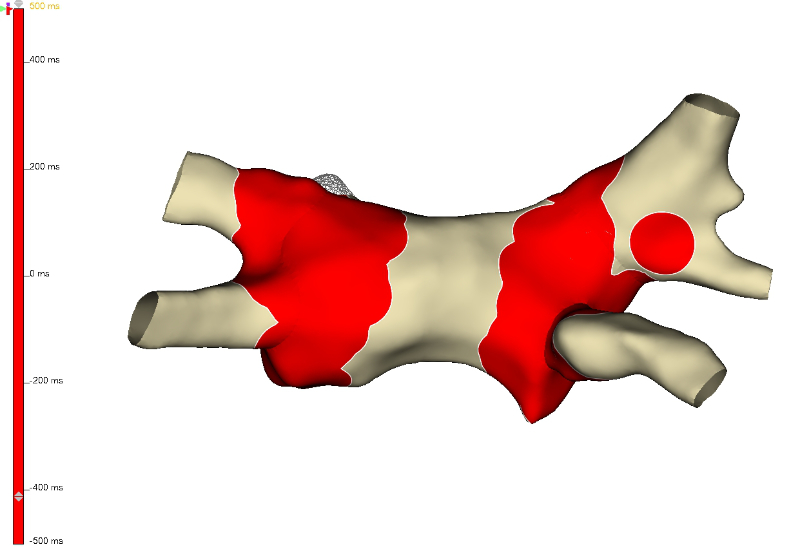
Here is a 3D electroanatomic map of the left atrium after a pulsed-field ablation, with the ablation sites in red. Note how broadly all 4 pulmonary veins are ablated, in a case which lasted less than 75 minutes overall.